
About 20 physicians and fellows — a mix of pediatricians, general internists, obstetrician-gynecologists, pathologists, nephrologists, and others — have arranged themselves around a U-shaped table in a small room on the Stanford campus. They are huddled together in groups talking quietly as instructor Kelley Skeff, MD, PhD, checks that everything is in order and then turns to the group and flashes a welcoming smile.
The physicians in this room have traveled from places as far flung as the Philippines and Tokyo to attend the fourth-annual Stanford 25 Skills Symposium, a two-day event dedicated to the promotion – and cultivation – of bedside medicine, and on this afternoon they are here to spend the next four hours learning how to improve their teaching at the bedside.
Skeff is just the man for the job. He has spent his career teaching physician-educators how to teach better, and how to train their colleagues back home to do the same. While many think of teaching as an innate gift, Skeff views it as a skill to be rigorously honed and improved. Alongside his colleagues at the Stanford Faculty Development Center, he has assessed, analyzed, and parsed over countless teacher-learner interactions, working to understand the seemingly nebulous concept of good medical teaching.
“What I’m going to do,” said Skeff, looking relaxed as he addressed the small crowd, “is to introduce you to the language we’ve created around the field of teaching, so you can both develop a methodology for thinking about teaching and have fun talking to each other about teaching... I hope you leave today with some ideas of what you want to do differently.”
Skeff’s ideas are organized into seven key categories that are both powerful and sensible, ranging from learning climate (“Which encapsulates the tone and atmosphere of the teacher setting. Is it stimulating? Would the learner want to be here?”) to clear communication of goals (“Ensuring that there is explicit understanding of a teacher’s expectations for the learner”). He illustrated these concepts using a series of mini-lectures, videos and group discussions.
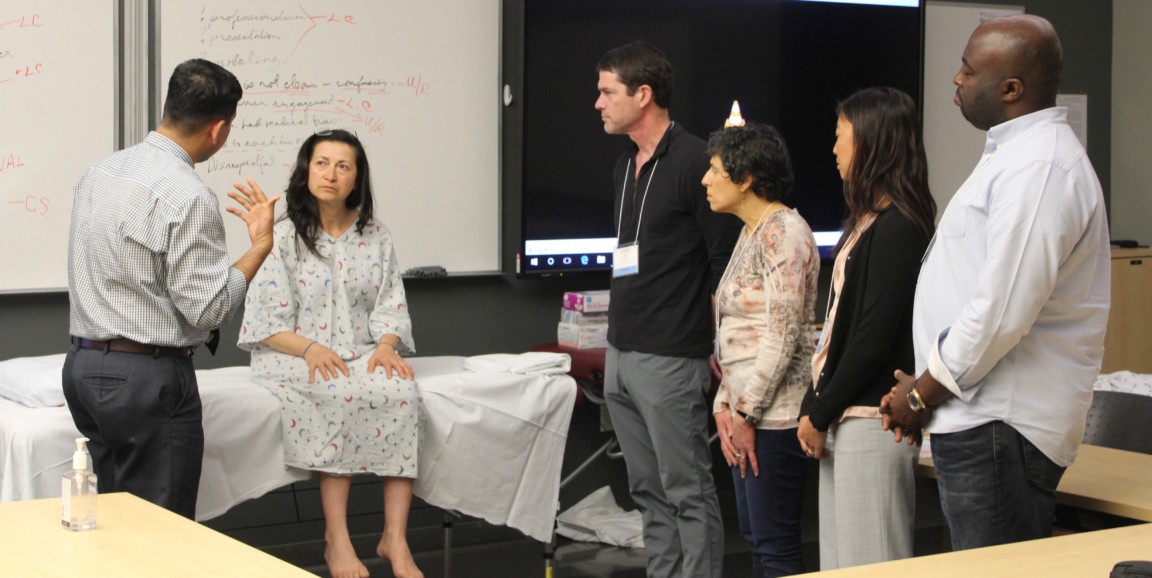
The group had a chance to employ Skeff’s lessons in a short role-playing scenario. Four participants — acting as an attending physician, resident, and learners — headed to the front of the room to meet a "patient" who was experiencing numbness and tingling in her arms that worsened at night.
Their first attempt goes well, but after a debrief the group identifies a few components that could change – including adding a short huddle with the care team to share information about what they know and don’t know before meeting the patient, slight tweaking of body language, and allowing several of the learners to interact and ask questions of the patient directly. The changes are small, yet the effect is remarkable. The care team feels united and cohesive, the learners feel included, and the patient reports feeling heard and respected.
Throughout the event, the attendees eagerly quiz Skeff, share stories about teaching triumphs, recall difficult learning experiences when they were medical students and residents and swap tips about how to engage learners — that four hours quickly pass, and it dawns on me that Skeff’s workshop is a testament to the effectiveness of his exceptional teaching philosophy. He has subtly employed every technique he has espoused to create a space that, in his own words, “is so vibrant, so open, and so safe that people can share and bring up what is really near and dear to their hearts.”
Photo by Lindsey Baker

